FAMILY | FUN | EMPATHY | CREATIVITY
Post Acute Centers

-
We have contracts with over 400 SNF centers in 7 states
-
We provide weekly RT support in over 200 centers
-
We run our Re-Hospitalization Intervention
-
Program (RHIP) in over 120 Centers
-
We run In-Patient Pulmonary Rehab Programs in over 40 Centers
PEL/VIP LTC Consulting

-
Provide Comprehensive Respiratory Services for all levels of PAC Care
-
Forge Partnerships with PACs by Providing: Education, Assessments & Recommendations, Standards of Care & Cost Saving Measures, Quality Measures
-
Increase Census Development with niche services targeting reduction of unplanned discharges
PEL/VIP Spaces

-
* Hospitals
-
* PAC (nursing adjunct, disease management, therapy, EQ-supplies)
-
* CCRC
-
* Out Patient Therapy
-
*Equipment/Safety in Home
-
*DME
-
Home Health
PEL/VIP- SUB ACUTE SERVICES:
-
Resident Assessment by a Licensed RT
-
Setup Equipment and Supplies
-
Education of Staff/Skills check-offs
-
Disease Management Programs:
-
Re-Hospitalization Intervention Program
-
In-Patient Pulmonary Rehab
-
Ventilator Unit Consulting & Outsourcing
-
Staffing Licensed RTs in SNFs
-
Provide Equipment Compliance Program
SKILLED NURSING FACILITIES:
Two types of Patients:
-
Skilled Patients requiring therapy (Med A, private pay payer source)
-
Patients requiring round the clock nursing care (Med B, Medicaid, private Insurance, private pay)
QUALIFYING FOR SNF CARE:
-
Medicare A patient with 3 noc hospital stay (patient eligible for 100 days in SNF)
-
MD writes an order for SNF Care
LTC PATIENT IN SNF
After patient reaches 100 days they may still need round the clock nursing care (ADL’s) they become a resident of center
RESPIRATORY THERAPY IN SNF’S
-
MDS pay for performance service (PPS) put respiratory therapy is under Nursing for reimbursement
-
PT, OT, SLP, Nursing have direct reimbursement
PEL/VIP AND SNF’S
-
2000’s PEL developed RT consulting in SNF’s (Assessments, In-Services, Trach Changes, Equipment Setups)
-
2005’s PEL developed disease management programs (Pulmonary Rehab, Re-Hospitalization Intervention Program)
-
2010’s PEL developed oxygen sales, equipment rental and sale, supplies, equipment compliance
-
2015’s PEL expanding our respiratory support (ACO’s, RT training, CMI Reimbursement)
2 TYPES OF PATIENTS WE SEE
Disease Management Patients:
-
PR
-
RHIP (Pneumonia, CHF, COPD)
Disease Management Patients:
-
One Time Assessment (maybe more depending upon situation)
-
Equipment Setup
* The Contract Determines How we see Patients!
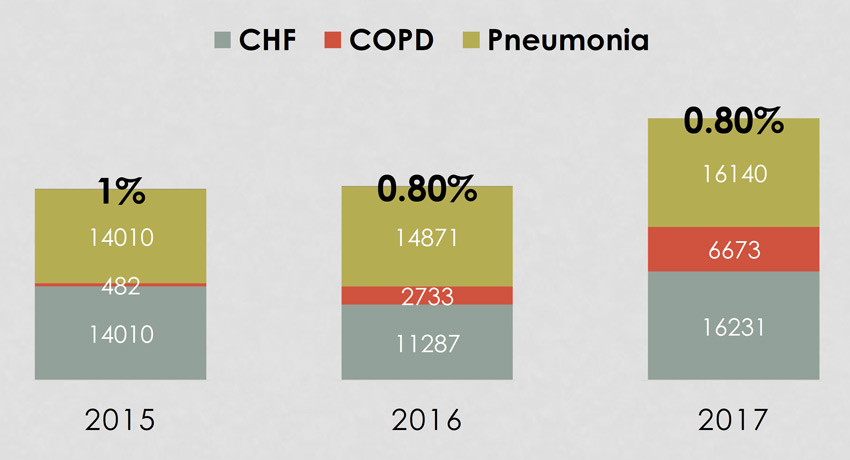
UNDER 2% RE-HOSPITALIZATION RATE FOR CHF, COPD & PNEUMONIA
-
Scoring Tools to gauge risk of recidivism
-
Care Pathways and Nursing Tasks based on acuity for each patient
-
Respiratory to assess, care plan, educate, assist with discharge
-
Monthly Outcome Reports for each PAC running program (RT will be emailed on monthly results)
-
Monthly Referral Report Summary
Customizable Data Collection
-
Disease Process
-
Referral Source
-
Risk for Re- Hospitalization
-
Payor Source
-
Length of Stay
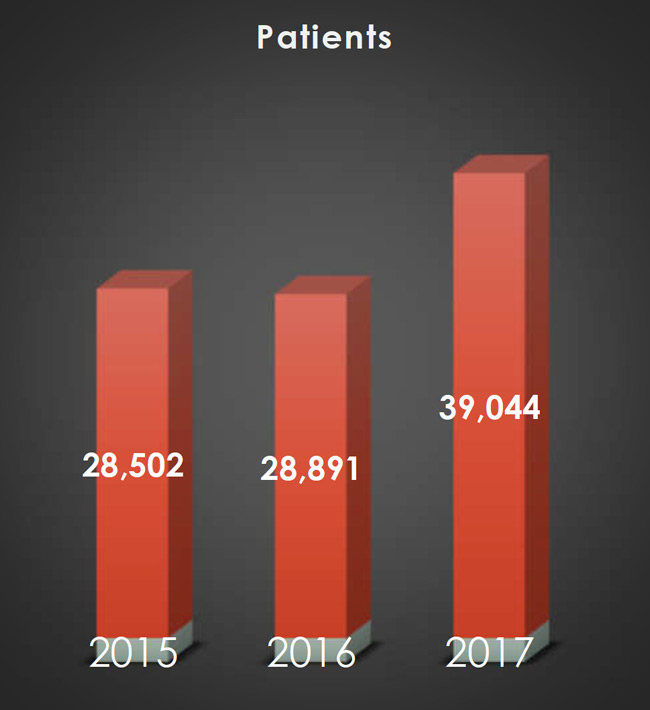
PEL/VIP PAC RE-HOSPITALIZATION RESULTS
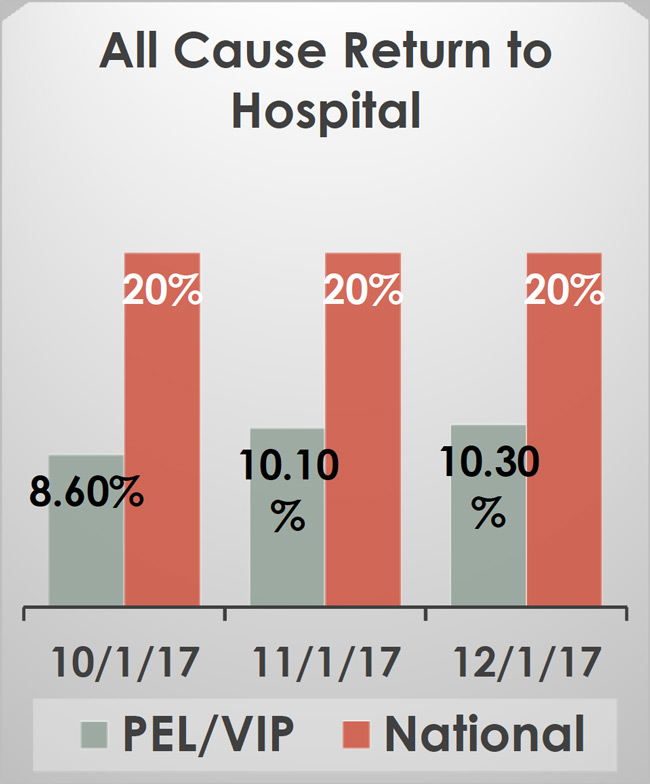
ALL CAUSE RETURN TO HOSPITAL
PEL/VIP 2017 Risk Adjusted All Cause Rate is 10.2%
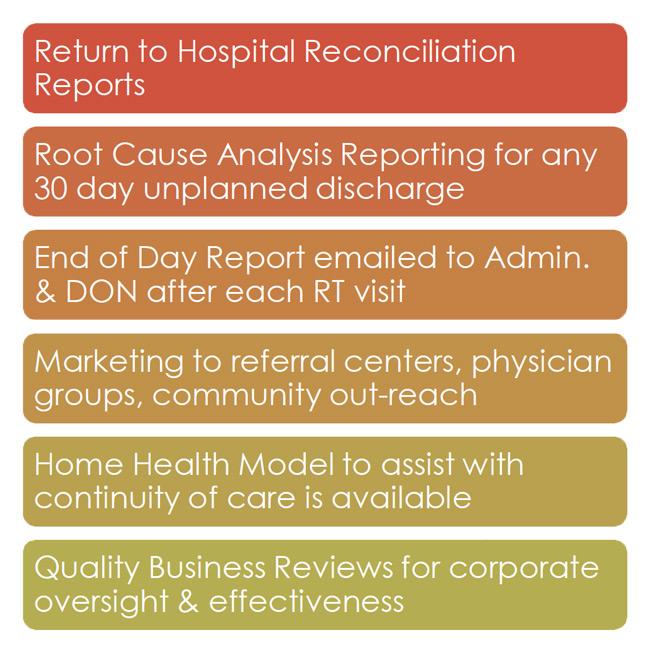
PEL/VIP Accountability Reporting
UNDER 2% RE-HOSPITALIZATION RATE FOR CHF, COPD & PNEUMONIA
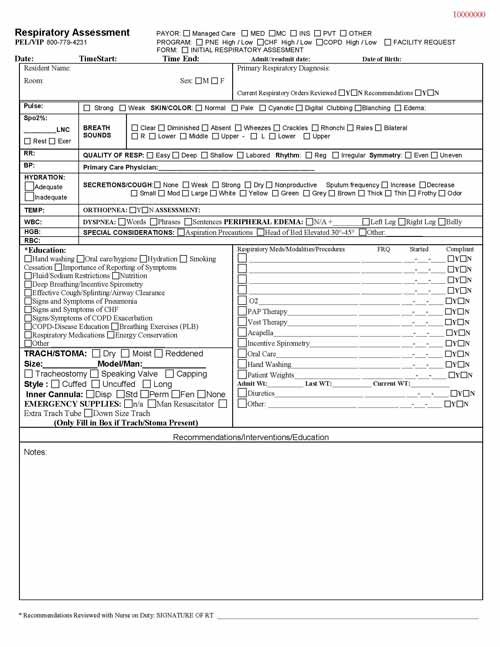
-
Used for every Initial Assessment
-
Used for all Disease management programs except (Orthopnea program)
ORTHOPNEA PROGRAM
-
To assist Centers in capturing Care Mix Index (CMI) for patients with COPD and their inability to lay Flat
-
New Program, not in very many centers